- Book Review: Where There is No Doctor and Other Resources
- Vitamin A Used in Treatment of Measles
- Electric Shock as First Aid for Poisonous Bites
- Reaction to Bee Stings
- Is the Africanized Bee Sting More Lethal Than That of Italian Bees?
- Do Mosquitoes Carry the AIDS Virus?
- Newsletter on AIDS
- Malaria Vaccine with Artemisia
- Homemade Mosquito Repellent from Neem
- Potential Contraceptive from Neem Tree Oil
- Oral Vaccine for Typhoid
- Effectiveness of a Moringa Seed Extract in Treating a Skin Infection
- Using Neem Leaves to Treat Scabies
- Honey as a Dressing for Wounds
- Don't Limit Calcium While Trying to Prevent Kidney Stones
- Review: Herbalgram
- CAB International (CABI) Health and Disease Publications
WHERE THERE IS NO DOCTOR AND OTHER RESOURCES. This book by David Werner is so widely used that most of you in the field probably already have a copy. An extremely useful health handbook for villages, it includes helpful signs in diagnosis and simple, basic treatments common in tropical situations. It is readable and easy to use, and would be a useful tool in health teaching. Copies are available at bookstores around the world and in several languages. If you cannot find it locally, write The Hesperian Foundation, P.O. Box 1692, Palo Alto, CA 94302, USA. You may also want to use other books in the same style and level of practicality: Where There is No Dentist, Disabled Village Children, and Helping Health Workers Learn. These are all handbooks which are both interesting and immediately applicable in your work.
VITAMIN A USED IN TREATMENT OF MEASLES. Don Mansfield with William Carey International University brought the following item in the Footsteps newsletter to our attention. "Children with severe measles do benefit from having a capsule of  vitamin A. Two studies from South Africa and Tanzania have shown that childhood mortality from measles can be reduced by about 30% if a capsule of 200,000 is given on each of two successive days. In fact, the World Health Organization recommends that this should be the routine management of measles where there is obvious vitamin A deficiency or where the proportion of children dying from episodes of measles exceeds 1%."
vitamin A. Two studies from South Africa and Tanzania have shown that childhood mortality from measles can be reduced by about 30% if a capsule of 200,000 is given on each of two successive days. In fact, the World Health Organization recommends that this should be the routine management of measles where there is obvious vitamin A deficiency or where the proportion of children dying from episodes of measles exceeds 1%."
Don adds, "In Mali we had kids die every year from measles. We had hundreds of bottles of vitamin A that had been donated. JoAnn just never knew to use it for measles. Maybe EDN can help get the word out to remote mission clinics."
ELECTRIC SHOCK AS FIRST AID FOR POISONOUS BITES. I received the following account of scorpion bites from Don and JoAnn Mansfield in Mali. Don works in agriculture; JoAnn runs the clinic.
"The missionary I replaced had told me how to treat scorpion stings with a pair of `electric shockers.' Frankly I did not believe it. Three weeks after we arrived a woman we knew came to the clinic. She had been stung on the side of her foot by a BIG scorpion of the kind that are common here. She was bent over with pain. We had nothing but an antihistamine, which did not 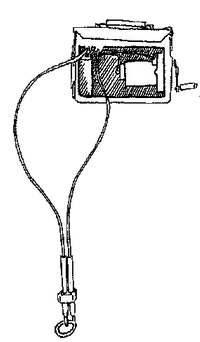 help. I told her about the shock treatment. She was in so much pain that she was willing to try anything.
help. I told her about the shock treatment. She was in so much pain that she was willing to try anything.
"We could not find the equipment my predecessor had told me about, but we did have a Briggs and Stratton power plant. I put the metal portion of the spark plug wire right on the spot where she had been stung, and had someone pull the rope. She jerked, but kept on moaning, hardly noticing the shock. The second pull had the same result. After the third pull she immediately straightened up, stopped moaning and began to leave. I stopped her and asked about the pain. She had none.
"In the next couple years we treated 4 or 5 more people similarly. In one case, where the sting was in a difficult spot to shock, there was still pain although it was a lot better. The others had total relief from pain, sometimes with one pull. None took more than three pulls."
Research into treating poisonous bites with electric shock began with Dr. Ron Guderian, a missionary in Ecuador, wondering about a widespread notion in Ecuador that electricity was therapeutic for snakebite. We wrote to Dr. Guderian for an update. A summary of his comments follow:
"In the laboratory we are trying to determine how the electric shock actually deactivates the venom, or what protein components the shock affects and how. This would give us the scientific basis to say how the shock works, not just that it appears to on trial." [The electric field changes the three-dimensional structure of the toxin, converting the venom to inert material. The shock eliminates the venom's biological activity.]
"We have been using the electric shock as a first aid measure for snake bites in Ecuador since 1980 and have found some very interesting results. If the shock treatment is given at the site of the bite and in an appropriate time frame, there is no reaction on the part of the person bitten." Shock has been used as first aid on the venomous bites of Portuguese men-of-war, Conga ants, scorpions, spiders, and even poison oak. It is used for snakes with hemotoxic venom which destroys blood cells and coagulation proteins, and does not have the same action on neurotoxic snakes (such as the cobra, mamba, and coral snakes).
"In the past two months we have treated several patients who have come to us 4-6 hours after being bitten. The site of the bite and surrounding tissues were edematous [Ed: in other words, venom had definitely been injected]. Having no other resource, the electric shock was given on the chance that it might help in some manner [Ed: Even though shock treatment is normally done much sooner than 4-6 hours]. To our surprise, the swelling decreased and in three days the site of the bite and surrounding tissues were normal. Without treatment, swelling usually increases and can last for weeks. The reduction is important because swelling causes much of the secondary complications from snake bites." In addition, the shock kills the anaerobic bacteria present in the bite which can lead to tissue death on the site.
THIS IS ONLY FOR USE IN REMOTE LOCATIONS WHERE ANTI-VENOM IS NOT AVAILABLE. "To answer your question, yes, shock should be used only if anti-venom is not available. Shock is not used along with anti-venom, nor in place of it. I have recorded 353 reports [by 1995] of the use of electrical shock with positive results."
TECHNICAL DETAILS. NEVER USE CURRENT FROM THE POWER COMPANY OR ALTERNATING CURRENT FROM YOUR OWN GENERATORS! "You need a DC pulsating electric current, 20-25 Kv and only milliamps of current. [An AC current can affect the heart; DC does not.] The best source of shock that we have found is the spark plug of an auxiliary gas motor such as a chain saw, motorcycle or outboard motor. Shock can also be applied directly from the coil of a car. Again let me say that this is experimental. The most important concept is that the patient be treated as soon as possible, preferably within 10-20 minutes. Otherwise permanent tissue damage may have already occurred.
"Most snake bites occur on the limbs. Ground the limb on the side opposite the bite. Hold the electrodes in place with tape as contact is otherwise broken during the discharge. Apply the shock directly to the bite for 2 seconds, rest and repeat 2-3 times depending on the size of the snake." [Don Stilwell with SIM sent us a summary of a conversation with Dr. Guderian 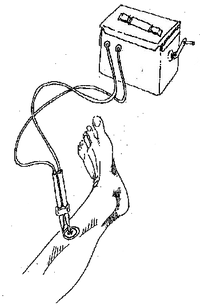 saying that the larger and more potent the snake and the more venom injected, the more shocks may be necessary, even up to eight discharges.]
saying that the larger and more potent the snake and the more venom injected, the more shocks may be necessary, even up to eight discharges.]
To be effective, the skin should be washed (with alcohol, if available) and dried; sweat is a good conductor. Ground the plate on the opposite side of the bite and apply the shock on the bite marks for best penetration of the skin (skin is very resistant, and 15,000-20,000 volts are needed to penetrate it). After this first aid is applied, send the patient to a medical center for evaluation. They should take 2 cc's of blood and put it in a clear tube undisturbed for 20 minutes. Tilt after 20 minutes; if a clot has formed, the patient should be fine. Repeat this test every 6 hours for 48 hours, and if clots still form, the patient may go home. If clots do not form, give antivenom; this may be necessary if treatment is delayed.
Dr. Guderian requests that, if you use this method, please keep a record of patients treated and note the type and location of bite, type of snake, time elapse between bite and treatment, source for current and patient's response. "Since we are still collecting data to prove that this method works in other parts of the world, I would appreciate receiving any such data." His address is Hospital Vozandes, HCJB Casilla 17-17-691, Quito, ECUADOR, South America; fax 593-2-447-263; e-mail rguderian@mhs.hcjb.com.ec. ECHO would like to know your results too.
REACTION TO BEE STINGS. The July 1987 issue of Florida's cooperative extension service bulletin on beekeeping, Apis, dedicated all four pages to the subject of reaction to bee stings (ask for a copy if you are very interested). The facts are even subject to controversy in the medical profession. The normal "local" reaction is "pain, swelling, redness, and itching... [such people are] at little risk of death unless the mouth or throat is affected so that the respiratory tract is obstructed." "Many people continue to believe that because they swell up they are at risk of losing their life when stung by bees. Ironically, it may in fact be the reverse. Those far more at risk may show no reactions to stings at all." It is systemic or allergic reactions that can be life-threatening. "There is no evidence that the very few who die as a result of a bee sting come from the pool of those who once before sustained a systemic reaction. On the contrary, no reaction at all may be a more ominous predictor of a lethal outcome on a subsequent sting." Stings inside the mouth and on the eyeball require special attention and are so very serious that when working with bees a veil should always be worn.
 Death usually comes from multiple causes, not simple anaphylactic shock or allergy. In fact, most allergic reactions are in children, while 90% of those who die of bee stings are over age 25. "One may readily see how (1) a hot summer day, plus (2) strenuous exercise, plus (3) coronary atherosclerosis, plus (4) a bee may add up to death, whether or not one invokes an allergic mechanism...." "Panic by the person stung or those around him/her can produce a systemic reaction in itself." "The frightening aspect of being stung cannot be ruled out as a cause of a systemic reaction. A patient who suddenly develops hives, shortness of breath (sometimes with bronchospasm) and giddiness ... is terrified, as are those about him. The patient may think he is going to die, as may his family or physician. What people need to know is that the vast majority of patients, particularly if aged under 25, will quickly recover. ... patients who have these terrifying experiences need to know that there is no evidence either that they came to the brink of death or that they are at greater risk of dying from a subsequent sting than anyone else."
Death usually comes from multiple causes, not simple anaphylactic shock or allergy. In fact, most allergic reactions are in children, while 90% of those who die of bee stings are over age 25. "One may readily see how (1) a hot summer day, plus (2) strenuous exercise, plus (3) coronary atherosclerosis, plus (4) a bee may add up to death, whether or not one invokes an allergic mechanism...." "Panic by the person stung or those around him/her can produce a systemic reaction in itself." "The frightening aspect of being stung cannot be ruled out as a cause of a systemic reaction. A patient who suddenly develops hives, shortness of breath (sometimes with bronchospasm) and giddiness ... is terrified, as are those about him. The patient may think he is going to die, as may his family or physician. What people need to know is that the vast majority of patients, particularly if aged under 25, will quickly recover. ... patients who have these terrifying experiences need to know that there is no evidence either that they came to the brink of death or that they are at greater risk of dying from a subsequent sting than anyone else."
The conclusion: "the risk of fatality ... is lower than previously thought. What must be emphasized, however, is that environmental factors and physical well being of the individual being stung cannot be ignored when judging who is at risk of dying from a bee sting. Nor can perceptions by the individual being stung. Panic by the person stung or those around him/her can produce a systemic reaction in itself.
IS THE AFRICANIZED BEE STING MORE LETHAL THAN THAT OF ITALIAN BEES? David Unander sent us a report in Nature which concluded that the lethality of Africanized ("killer") bees is entirely due to their tendency to attack in mass. In South and Central America colony defenses result in attacks during which thousands of stings may be inflicted on one individual. "Although attacks of 300-500 stings have been survived without treatment, more than 500 stings are commonly fatal." Venom was collected from worker honeybees in Arizona and Africanized bees in Costa Rica. Analysis of venom pooled from 1,000 bees of each type showed that European bees contained more venom (145 micrograms dry weight) than the smaller Africanized bees (94 micrograms). In a trial with mice, the lethal dose for the purified venom was identical for both kinds of bees with one strain of mice. For the other strain of mice, the dose of Africanized bee venom required to have the same effect as honeybee venom was considerably higher (7.1 vs 4.6 mg/kg).
DO MOSQUITOES CARRY THE AIDS VIRUS? In case you are worrying about this frequent rumor, the following is quoted from World Development Forum, November, 1986. "The Pasteur Institute's Jean-Claude Chermann, a co-discoverer of the AIDS virus in 1983, says they do. A study in Zaire of 50 insects, reports Asia Week, indicated that all--including mosquitoes, tsetse flies and cockroaches--were infected. But the reassuring news is that the 'insects don't carry nearly enough of the virus to infect a human.' There is no way, he said, that the virus could be transmitted to humans by mosquitoes or other insects."
NEWSLETTER ON AIDS in Latin America. Bolet¡n SIDA is a Spanish language bulletin published three times a year by MAP-Latin America. "We have produced this bulletin to inform the Evangelical churches in Latin America about the advance of the disease, its consequences, the methods of prevention, treatment and accompanying emotional issues for those affected. We hope to stimulate the church to take part in the struggle against AIDS." To subscribe (no charge, but donations welcome) send them your name and address. Also mention the kind of work you do and whether your work currently involves you in AIDS issues. Write MAP, Bolet¡n SIDA, Casilla 17-08-8184, Quito, ECUADOR; phone (593-2) 452-373; fax (593-2) 435-500.
MALARIA VACCINE WITH ARTEMISIA. Because malaria is caused by a protozoan (a small animal) rather than bacteria or a virus, a vaccine has been difficult to develop. Experiments in Colombia suggest that it may be possible, however. They synthesized several polypeptides which are identical to segments of proteins on the protozoan. (Proteins are very large polypeptides.) Monkeys inoculated with the right mixture of these polypeptides developed partial to complete immunity to malaria. It has not yet been tried in humans. If you want a copy of the article let us know. (It is pretty heavy biochemistry.)
 The following is abstracted from World Watch, May/June 1994. "More than 20 years ago Chinese scientists confirmed the antimalarial qualities of artemisinin, ... extracted from a fern-like plant Artemisia annua." This plant has been used as an anti-malarial drug for more than 1,500 years. Now derivatives of artemisinin that can be taken orally or injected have been developed and are widely used in Southeast Asia, and in parts of Africa and Latin America. The injectable form acts more rapidly than any other antimalarial and is effective against multi-drug-resistant parasites. It is not yet approved in any developed country.
The following is abstracted from World Watch, May/June 1994. "More than 20 years ago Chinese scientists confirmed the antimalarial qualities of artemisinin, ... extracted from a fern-like plant Artemisia annua." This plant has been used as an anti-malarial drug for more than 1,500 years. Now derivatives of artemisinin that can be taken orally or injected have been developed and are widely used in Southeast Asia, and in parts of Africa and Latin America. The injectable form acts more rapidly than any other antimalarial and is effective against multi-drug-resistant parasites. It is not yet approved in any developed country.
The article in World Watch says that clinical trials have now been done and that "40-66% of participants were protected from the most common and deadly strain, Plasmodium falciparum, which is responsible for 95% of malaria cases." "Although Patarroyo's initial field trials were criticized because they did not meet international protocols, he answered their skepticism by conducting trials that did meet those standards. One of those trials, completed in 1992 in Ecuador, showed that the vaccine was successful in protecting 66% of the volunteers from the common malaria strain." It has been tested on 41,000 people in South America. Finally the World Health Organization and the Walter Reed Army Institute of Research are beginning tests in Africa and Asia.
"Meanwhile, other researchers are ... studying the feasibility of altering the mosquito's genetic makeup so that it will be unable to carry and transmit the parasite to humans." [Presumably this mosquito would compete with normal mosquitos for food and breeding grounds, so the number capable of infecting people would drop.]
HOMEMADE MOSQUITO REPELLENT FROM NEEM. Dr. V.P. Sharma, Director of the Malaria Research Centre in New  Delhi, says the repellent is particularly effective against the Anopheles mosquito which spreads malaria. When the preparation is applied to the body, mosquitoes are effectively repelled. Low-cost neem oil is mixed with coconut oil in concentrations of 1-2%. This information is taken from Neem News, vol 1, p. 4, published by the Neem Association, 1511 Oneco Ave., Winter Park, FL 32789, USA. The non-profit association is organized to promote communication between neem scientists, growers and producers; promote its various uses and seek other uses; promote research to develop superior varieties of neem and to develop new uses.
Delhi, says the repellent is particularly effective against the Anopheles mosquito which spreads malaria. When the preparation is applied to the body, mosquitoes are effectively repelled. Low-cost neem oil is mixed with coconut oil in concentrations of 1-2%. This information is taken from Neem News, vol 1, p. 4, published by the Neem Association, 1511 Oneco Ave., Winter Park, FL 32789, USA. The non-profit association is organized to promote communication between neem scientists, growers and producers; promote its various uses and seek other uses; promote research to develop superior varieties of neem and to develop new uses.
POTENTIAL CONTRACEPTIVE FROM NEEM TREE OIL. I do not normally include items in EDN that are not yet ready for use. Because we have mentioned neem so often, though, I thought you would be interested in this item taken from Agroforestry Today. Indian scientists have isolated a neem oil extract which they believe can be refined into a birth control agent for women. They report it has spermicidal qualities and also can prevent a fertilized egg from being implanted in the uterus, possibly by interfering with estrogens. Unfortunately their "ultimate aim is to refine it into a powder that can be synthesized in the laboratory." I hope someone follows up to see whether a technique might be developed for making contraceptives directly from neem in a simple laboratory that could be set up anywhere.
ORAL VACCINE FOR TYPHOID. When I think of typhoid shots I think of finding time for three trips to a doctor, major soreness and some fever. A trip that comes up suddenly often does not allow time for completing the series. So when Glen Munro told me that he was immunized with no noticeable side effects by taking four pills, one every other day, I asked for details. He said the immunity is supposed to last 5 years. The series cost him $30. It is a live vaccine and must be refrigerated at all times. It is manufactured by the Swiss Serum and Vaccine Inst., Berne, Switzerland. I contacted Andy Murai at their U.S. subsidiary, Berna Products Corporation, 4216 Ponce de Leon Blvd., Coral Gables, FL 33146; phone 800/533-5899 or 305/443-2900; fax 305/567-1043. He said they are glad to ship overseas, even if orders are small.
EFFECTIVENESS OF A MORINGA SEED EXTRACT IN TREATING A SKIN INFECTION. There are powerful antibiotic  and fungicidal effects of pterygospermin from the flowers and roots of the moringa tree. Now Axel Bosselmann has brought to our attention a study by Drs. Caceres and Lopez at the University of San Carlos in Guatemala. The article is summarized below.
and fungicidal effects of pterygospermin from the flowers and roots of the moringa tree. Now Axel Bosselmann has brought to our attention a study by Drs. Caceres and Lopez at the University of San Carlos in Guatemala. The article is summarized below.
Herbal applications are commonly used to treat skin infections in developing countries, although few investigations are conducted to validate scientifically their popular use. The small drought-resistant Moringa oleifera tree produces edible leaves, pods, flowers and roots. A previous study had showed that seeds are effective against skin infecting bacteria Staphylococcus aureus and Pseudomonas aeruginosa in vitro (i.e. in a test tube). This study showed that mice infected with S. aureus recovered as quickly with a specially prepared aqueous extract of moringa seed as with the antibiotic neomycin.
This study proves only the effectiveness of moringa as they prepared it. That preparation could be done in any country, but not with just household utensils. It was prepared by infusing 10 g powdered moringa seeds in 100 ml of 45 deg.C water for 2 hours. The part that is a bit more complicated is reducing the 100 ml down to 10 ml by placing it in a rotavaporator. This is a very common piece of laboratory equipment which continually rotates a flask containing the liquid. An aspirator attached to a faucet produces a modest vacuum when the water is turned on. A rubber tube from the aspirator is connected to the rotavaporator, reducing the pressure and causing the water to evaporate rather quickly without boiling it. The ointment was prepared by placing 10% of the extract in vaseline. (We can send a copy of the article to medical personnel.)
Are you in a situation where there is a shortage of antibiotics? This ointment could be prepared for use in the local community anyplace where there is electricity and running water. I would not be surprised if much simpler methods, better suited to preparation as needed in the home, might not also be effective. I hope someone will devise and test such preparations.
USING NEEM LEAVES TO TREAT SCABIES. Larry Radice, of Maryknoll Fathers and Brothers in Tanzania, wrote, "After reading in EDN about use of moringa to treat a skin infection, I thought I might share with you and your readers my experience using neem tree leaves to treat scabies. (Scabies, also called seven year itch, is especially common in children. It causes very itchy little bumps that can appear all over the body, but are most common between fingers, on wrists, the waist and genitals. It is caused by little animals similar to tiny ticks or chiggers, which tunnel under the skin.)
"I lived in Tanzania for almost 8 years. One day while visiting a friend's home I noticed his daughter had a very bad case of scabies. ... I was told that she had gone to the local clinic, bought some medicine, but it had run out and the scabies had not cleared up. ... Her scalp was horribly encrusted and she had no hair in the infected area.
"I knew that neem tree leaves had insecticidal properties and that scabies is caused by a small mite. So I thought it would be worth a try.... I had the mother take neem tree leaves, about a hand full, and pound them into a mush adding a bit of water. I believe she then heated this, boiling off the excess water and leaving a paste. I told her to apply the poultice to the infected area twice a day for five days, leaving it to dry on the scalp.
"When I visited the home again two weeks later I had hardly said hello before she was excitedly telling me that her daughter was well. In fact by the third day the scabies was drying and by the end of that first week she could see new hair growing.  When I saw the child the scabies were gone. I suggested the cure two other times and in both cases I later heard that the scabies had cleared up, but I did not get to see those results for myself."
When I saw the child the scabies were gone. I suggested the cure two other times and in both cases I later heard that the scabies had cleared up, but I did not get to see those results for myself."
In response to this letter, Dr. S. X. Charles at the Medical and Cancer Research and Treatment Center in India sent us the results of a study of 814 people treated with neem and turmeric. Scabies is normally treated with a scrub bath, boiling the fomites (clothes and bed linens), and application of benzyl benzoate. "The drug caused skin reaction when rubbed on the face, and children accidentally rubbing it ... in the eyes was common." Where There is No Doctor recommends a homemade but dangerous alternative to those who cannot afford the benzyl benzoate. In this, the very toxic insecticide lindane is mixed with 15 parts of vaseline. The neem method is far less toxic and essentially free.
"Fresh neem leaves and turmeric are ground to a paste in the proportion of 4:1 by weight. The measurement that is taught to mothers is a handful of neem leaves and a piece of turmeric 1/2 the length of the index finger. This paste is rubbed all over the body and left to dry. The procedure is repeated daily until the patient is cured. (Boiling clothes and scrub bath is carried out daily before application of the paste.)
"Paste rubbed on the face has not caused any skin reaction or other toxic symptoms. Because of the bitter taste, chances of children swallowing it was remote, and even if swallowed [is not toxic]." "Of the 824 cases, 98% showed complete cure within 3-15 days of treatment. Those cases (95.8%) with localized lesions showed cure in 3-5 days. When lesions were all over the body and there was secondary infection, treatment needed for a cure was 6-15 days. Failure of treatment was only 2%. The reasons for failure were irregular application of paste and not doing the preliminary treatment of scrub bath and boiling of fomites to prevent reinfection."
HONEY AS A DRESSING FOR WOUNDS. (Based on an article in the October 1992 issue of Apis.) New Zealand bee scientist Dr. Peter Molan says that "honey is used in many countries in the treatment of burns, blisters, bed sores and major wounds. Honey has long been used as a wound dressing and is probably the perfect substance for such a use. Not only is it antibiotic (killing almost all bacteria), it also keeps the wound from dehydrating. Almost all other wound dressings either keep the wound dry (avoiding infection, but leading to scarring), or moist (avoiding the severe effects of dehydration, but making a great medium for bacteria to grow).
"Honey is also better than man-made antibiotics, Dr. Molan contends, because such antibiotics actually slow down the rate of cell growth. The moisture-attracting nature of honey, on the other hand, pulls body fluids and nutrients to the wound surface where they help speed skin growth and healing."
"All honey gives off hydrogen peroxide, a known antibiotic. The hydrogen peroxide is produced when the glucose in honey reacts with oxygen. The problem with peroxide as an antibiotic is that in large concentrations it breaks down in the presence of a common enzyme, producing the characteristic fizz we see when we put it on a cut. Because it is produced slowly in honey, at a low level, the peroxide doesn't loose its effectiveness. Provided honey is kept away from light, the enzyme which breaks down the hydrogen peroxide won't even activate."
Dr. Molan has now discovered a second antibacterial property, present in some but not all New Zealand honey. It has been shown to be effective against Helicobacter pylori, which is thought to be the major cause of stomach ulcers. Tests will begin soon in which patients will be given a tablespoon of this honey five times a day. This substance also works against highly resistant bacteria such as the MSRA bacterium which is gaining a reputation for closing down hospital wards.
DON'T LIMIT CALCIUM WHILE TRYING TO PREVENT KIDNEY STONES. (Adapted from Science News, Vol 143, March 27, 1993.) Most kidney stones are made up of crystals of calcium and a naturally- occurring substance in some plants called oxalates. Many plants contain such high amounts of oxalates that we must temper our enthusiasm for those plants. Amaranth leaves and carambola fruit are good examples.
The conventional wisdom is that people with kidney stones should cut back on calcium in their diet. According to a study reported in the New England Journal of Medicine, men who ate a diet rich in calcium had a 34% lower risk of kidney stones than men who followed a restricted calcium diet.
"This goes against everything we have been taught," said one of the authors, kidney specialist Gary Curhan. He suggests that the reason may be that oxalates in the diet combine with calcium in the intestine in normal diets, creating insoluble crystals that are excreted. A low calcium diet would allow more oxalate to enter the bloodstream and eventually form insoluble crystals with calcium in the kidneys.
 Dr. Curhan is not recommending added calcium, but that calcium not be reduced. I cannot help but wonder, though, whether taking extra calcium when I am going to be eating high oxalate foods might result in more of the oxalates being excreted harmlessly.
Dr. Curhan is not recommending added calcium, but that calcium not be reduced. I cannot help but wonder, though, whether taking extra calcium when I am going to be eating high oxalate foods might result in more of the oxalates being excreted harmlessly.
On a side note, the same study also found that men who ate a potassium-rich diet had a 50% lower risk of stones than those who ate the least amount of potassium. Bananas, oranges and grapefruit are good sources of potassium.
HERBALGRAM is the journal of the American Botanical Council and the Herb Research Foundation. For those interested in botany and pharmacology, this will make a fascinating read. Articles often discuss toxicities and traditional medicinal uses of various plants, with a chemical-scientific focus. We often find an interesting but otherwise obscure abstract about a new use for one of the tropical plants we have on ECHO's farm. The book list is unbelievable; we often wish we had the budget to buy everything on the page! Subscriptions are $25/year, $60/3 years; foreign subscriptions add $10/year. Write the American Botanical Council, P.O. Box 201660, Austin, TX 78720, USA; phone 512/331-8868; fax 512/331-1924.
CAB INTERNATIONAL (CABI) HEALTH AND DISEASE PUBLICATIONS provide up-to-date medical information on a wide variety of topics. (CABI also works with agriculture, forestry, and natural resource management in developing countries.) The latest catalog mentions a new health and disease database which covers parasitology, tropical diseases, communicable diseases, human nutrition, public health, and medicinal and poisonous plants. The catalog lists newsletters, journals, books, and computer resources. Items listed are expensive, but this is a good resource for those needing specific medical information on a variety of health problems in tropical countries. Request information from CAB International, Wallingford, Oxon OX10 8DE, UK; phone (01491)832111; fax (01491)883508; e-mail cabi@cabi.org; http://www.cabi.org/.